
🩺 Understanding Rubber Band Ligation for Hemorrhoids
Hemorrhoids are swollen vascular structures in the anal canal, and while they’re extremely common, the MCAT and clinical exams love testing the difference between internal and external hemorrhoids. Rubber band ligation is the most widely used procedure for treating internal hemorrhoids, and King of the Curve’s visual breaks down exactly how the technique works. This minimally invasive method deprives the hemorrhoid of blood flow, causing it to shrink and eventually fall off.
🔍 What Exactly Are Internal Hemorrhoids?
Internal hemorrhoids arise above the dentate line, meaning they are generally painless due to visceral innervation. Patients typically present with painless rectal bleeding, prolapse, or mucus discharge. Because they lack somatic pain fibers, internal hemorrhoids are ideal candidates for rubber band ligation a treatment that would be far too painful for external hemorrhoids located below the dentate line.
🧰 How Rubber Band Ligation Works
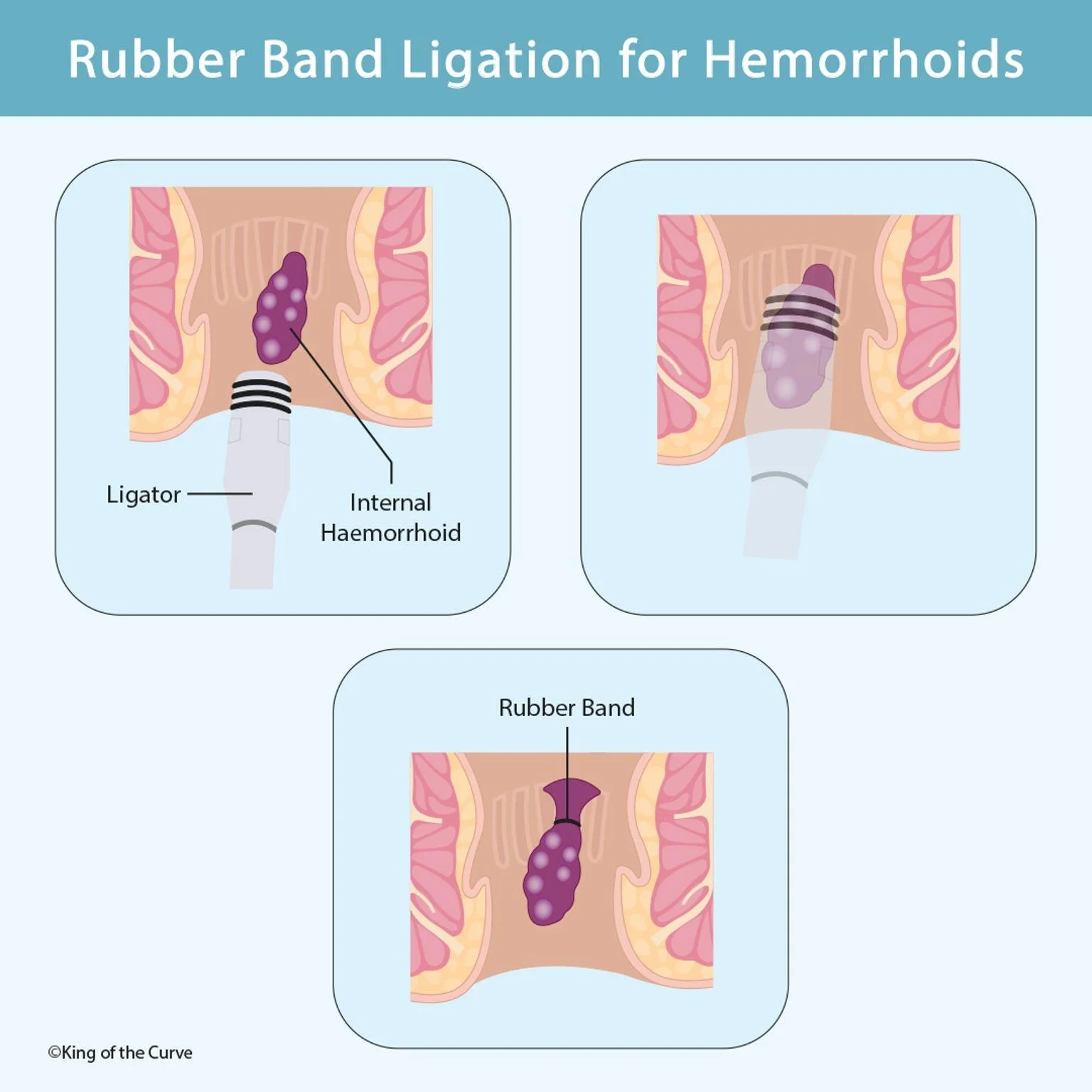
During the procedure, a device called a ligator is inserted into the anal canal. The internal hemorrhoid is suctioned or grasped into the instrument, and a small rubber band is placed around its base. This band cuts off the blood supply, leading to ischemia. Over several days, the hemorrhoid shrivels and falls off naturally during bowel movements.
🔄 What Happens After the Band Is Placed
Once circulation is cut off, the hemorrhoid begins to darken and shrink. Patients may feel a sensation of fullness or mild discomfort, but significant pain usually indicates that the band was placed too low. Within 3–7 days, the hemorrhoid sloughs off, leaving behind a small ulcer that heals on its own. The goal is to minimize bleeding and prevent prolapse without requiring surgical excision.
📊 High-Yield Table: Rubber Band Ligation
| Topic | Key Points | MCAT Relevance |
|---|---|---|
| Indication | Internal hemorrhoids (grades I–III) | Differentiating internal vs. external |
| Mechanism | Cuts blood supply → necrosis → hemorrhoid detaches | Ischemia and tissue death concepts |
| Pain Level | Minimal (above the dentate line) | Nervous system: visceral vs. somatic |
| Complications | Mild discomfort, bleeding, infection (rare) | Recognizing red flags in clinical vignettes |
🧠 Why MCAT Students Should Know This
The MCAT frequently tests anatomy of the anal canal, innervation patterns, and the clinical behavior of hemorrhoids. Rubber band ligation is a perfect example of how anatomical boundaries dictate treatment options. Understanding why this procedure works for internal but not external hemorrhoids reveals deeper principles about pain pathways, vascular supply, and gastrointestinal physiology.
📚 Using KOTC Visuals to Master Clinical Anatomy
KOTC’s graphical breakdown of rubber band ligation simplifies a procedure that students often find abstract. Pairing these visuals with our Adaptive Q-Bank and daily science questions at kingofthecurve.org/studyscience will reinforce your understanding of GI anatomy and make clinical scenarios much more intuitive. Clear visuals lead to clearer thinking especially on test day.

Frequently Asked Questions (FAQs)
-
Aim for 4-6 focused hours, ensuring you incorporate breaks to avoid burnout.
-
Practice mindfulness techniques, take practice exams under realistic conditions, and maintain a balanced lifestyle.
-
Set short-term goals, seek support from mentors, and reward yourself for small achievements.
-
Regular exercise improves focus, reduces stress, and enhances overall mental clarity.
-
KOTC offers personalized learning tools, gamification features, and adaptive question banks to help students stay on track without burnout.