
🧪 Differential Diagnosis of Metabolic Alkalosis
Metabolic alkalosis is a common acid-base disorder characterized by an increase in blood pH above 7.45 along with elevated serum bicarbonate (HCO₃⁻ > 24 mEq/L). It typically arises due to loss of hydrogen ions, excessive bicarbonate retention, or volume depletion. Understanding the underlying cause is essential for effective treatment, and one of the most practical ways to approach this condition is by evaluating urine chloride levels.
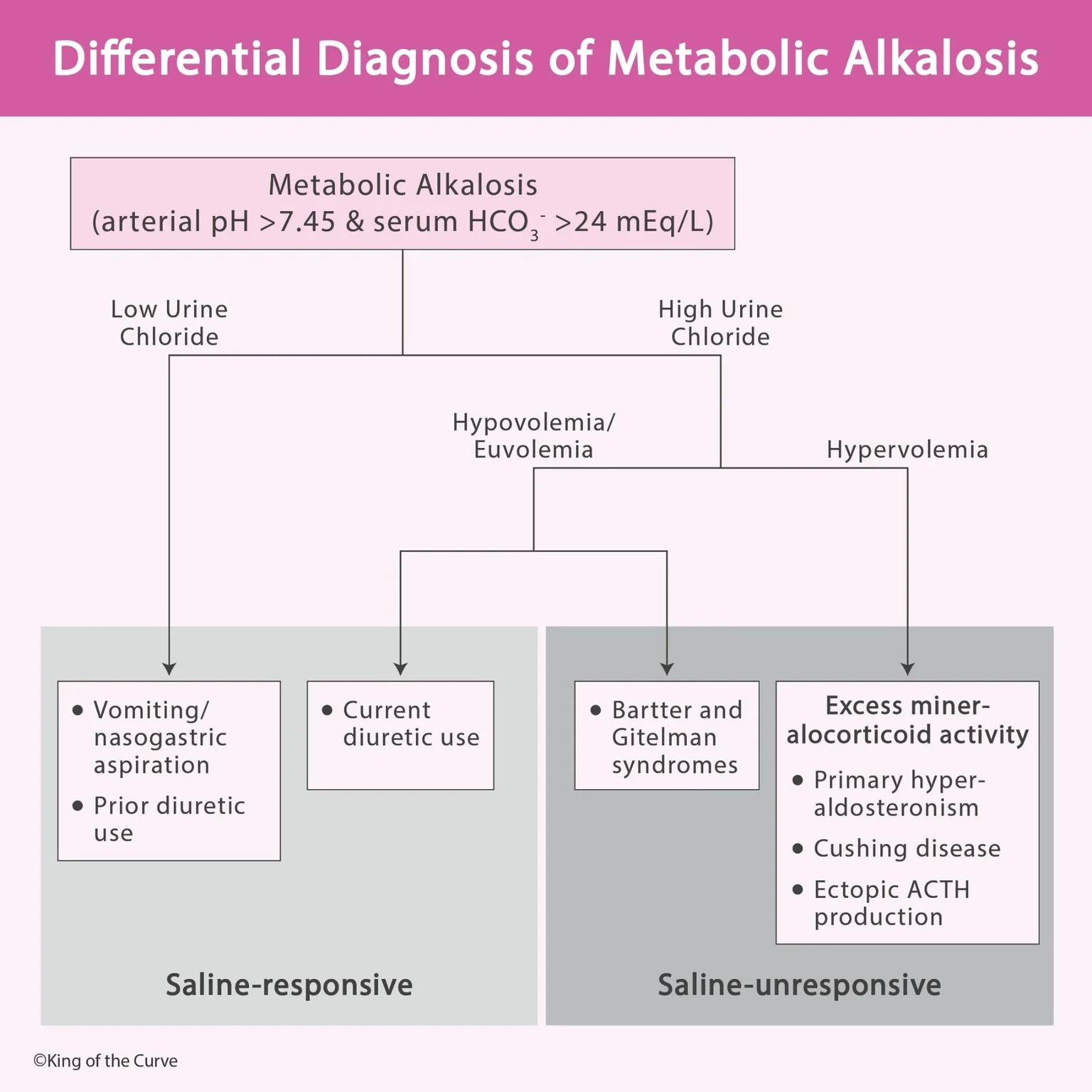
🔍 Step 1: Assess Urine Chloride
Urine chloride is the key initial test in evaluating metabolic alkalosis. It helps divide causes into two main groups:
Low urine chloride (<10–20 mEq/L): Suggests chloride depletion
High urine chloride (>20 mEq/L): Suggests ongoing renal loss or mineralocorticoid activity
This distinction is crucial because it determines whether the condition will respond to saline therapy.
💧 Saline-Responsive Metabolic Alkalosis
When urine chloride is low, the condition is typically saline-responsive, meaning it improves with volume and chloride replacement.
Common Causes:
Vomiting or nasogastric suction: Loss of gastric acid leads to alkalosis
Prior diuretic use: Causes volume depletion and secondary alkalosis
In these cases, the body is trying to conserve chloride, resulting in low urinary chloride levels. Treatment usually involves normal saline and potassium replacement, which restores volume and corrects the alkalosis.
⚖️ Saline-Unresponsive Metabolic Alkalosis
When urine chloride is high, the condition is saline-unresponsive, indicating that simply giving fluids will not correct the problem.
Hypovolemia / Euvolemia Causes:
Current diuretic use: Ongoing renal loss of sodium and chloride
Bartter syndrome
Gitelman syndrome
These conditions involve renal tubular dysfunction leading to persistent electrolyte loss.
Hypervolemia Causes:
Excess mineralocorticoid activity, including:
Primary hyperaldosteronism
Cushing disease
Ectopic ACTH production
These disorders increase sodium retention and potassium/hydrogen loss, maintaining alkalosis despite adequate volume.
⚠️ Role of Electrolytes and Potassium
Potassium levels play a crucial role in the development and maintenance of metabolic alkalosis. Hypokalemia (low potassium) often accompanies alkalosis and further worsens it by promoting hydrogen ion loss from cells. This creates a cycle where alkalosis and hypokalemia reinforce each other. In conditions like diuretic use, Bartter syndrome, or hyperaldosteronism, potassium depletion is a key feature, making potassium replacement an essential part of management alongside treating the underlying cause.
🧾 Importance of Clinical History
A thorough clinical history is vital when interpreting metabolic alkalosis. Factors such as recent vomiting, use of diuretics, blood pressure status, and signs of endocrine disorders can significantly narrow the diagnosis even before laboratory results are available. For example, a hypertensive patient with metabolic alkalosis and high urine chloride strongly suggests mineralocorticoid excess, whereas a patient with a history of vomiting and low urine chloride points toward volume depletion. Combining clinical clues with laboratory findings ensures a more accurate and efficient diagnosis.
📊 Summary Table
| Category | Urine Chloride | Volume Status | Common Causes | Treatment |
|---|---|---|---|---|
| Saline-responsive | Low | Hypovolemia | Vomiting, prior diuretics | IV saline + K⁺ |
| Saline-unresponsive | High | Hypo/Euvolemia | Bartter, Gitelman, active diuretics | Treat underlying cause |
| Saline-unresponsive | High | Hypervolemia | Hyperaldosteronism, Cushing, ACTH | Hormonal management |
🧠 Clinical Insight
The distinction between saline-responsive and saline-unresponsive metabolic alkalosis is not just academic—it directly impacts treatment decisions. While saline-responsive cases improve rapidly with fluid resuscitation, saline-unresponsive cases require targeted therapy aimed at correcting hormonal or renal abnormalities.
🩺 Key Takeaway
Always start with urine chloride measurement when evaluating metabolic alkalosis. This simple test can quickly narrow down the differential diagnosis and guide effective treatment, saving time and improving patient outcomes.

Frequently Asked Questions (FAQs)
-
Aim for 4-6 focused hours, ensuring you incorporate breaks to avoid burnout.
-
Practice mindfulness techniques, take practice exams under realistic conditions, and maintain a balanced lifestyle.
-
Set short-term goals, seek support from mentors, and reward yourself for small achievements.
-
Regular exercise improves focus, reduces stress, and enhances overall mental clarity.
-
KOTC offers personalized learning tools, gamification features, and adaptive question banks to help students stay on track without burnout.