
🧪 Salivary Composition and Secretion: From Isotonic to Hypotonic
Saliva is more than just water it is a carefully regulated fluid essential for digestion, oral health, and protection against pathogens. Its composition changes as it moves through the salivary glands, transforming from an isotonic plasma-like solution into hypotonic saliva before entering the mouth.
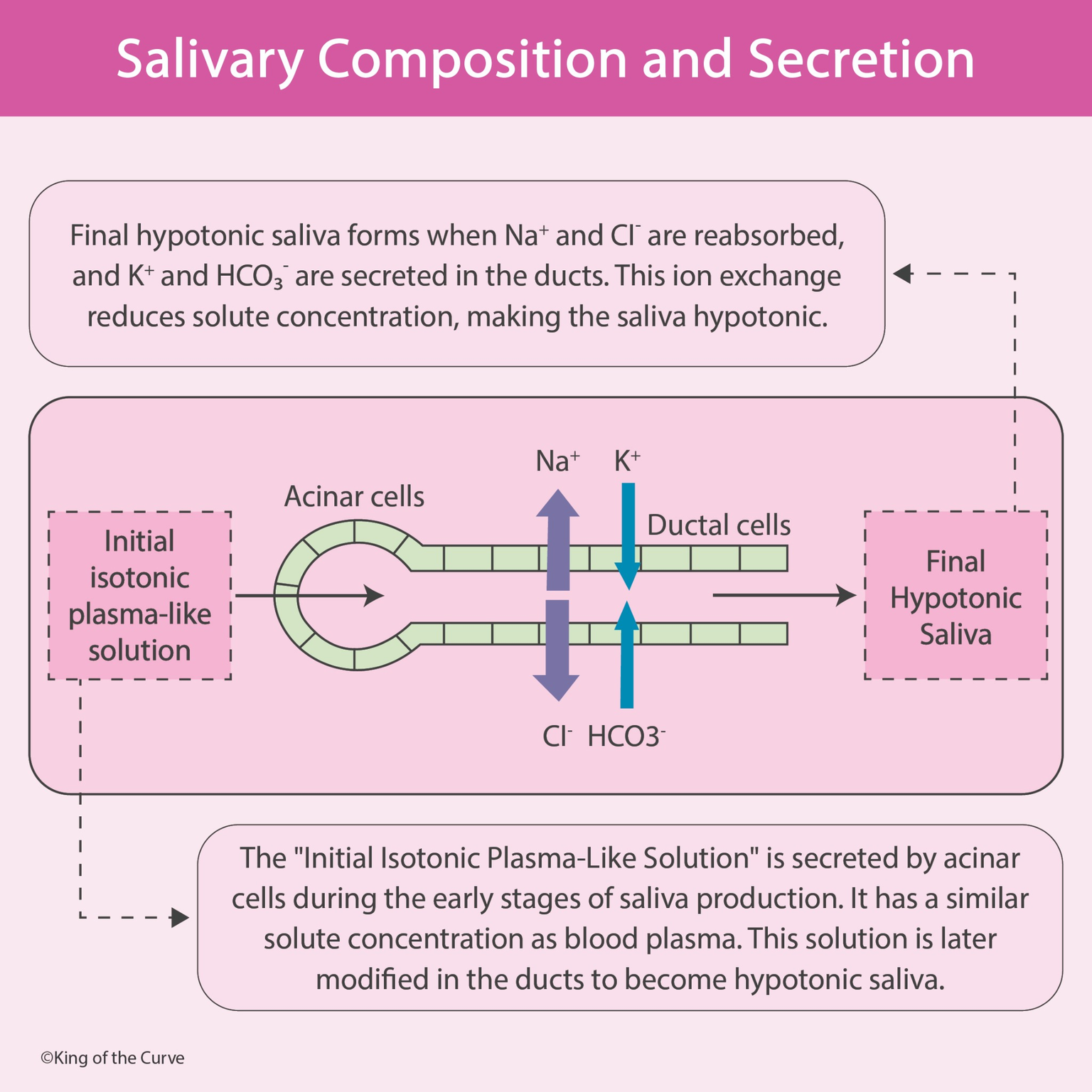
🧪 Step 1: Formation of Initial Isotonic Saliva
Saliva production begins in the acinar cells of the salivary glands.
These cells secrete a fluid that closely resembles blood plasma in osmolarity. This early secretion contains:
Sodium (Na⁺)
Chloride (Cl⁻)
Water (H₂O)
Small amounts of potassium (K⁺)
Bicarbonate (HCO₃⁻)
Because water moves freely across acinar cell membranes, the fluid produced is isotonic — meaning it has a similar solute concentration to plasma.
This is called the primary saliva.
🔄 Step 2: Modification in the Ductal Cells
As the primary saliva travels through the ductal cells, its composition changes significantly.
Ductal cells:
Reabsorb Na⁺ and Cl⁻
Secrete K⁺ and HCO₃⁻
Are relatively impermeable to water
Since water cannot follow the reabsorbed sodium and chloride, the total solute concentration decreases while water content remains unchanged.
This is the key reason saliva becomes hypotonic.
💧 Why Final Saliva Is Hypotonic
The final saliva entering the oral cavity has:
Lower Na⁺ and Cl⁻ levels
Higher K⁺ and HCO₃⁻ levels
Reduced overall osmolarity compared to plasma
Because solutes are removed but water remains, the fluid becomes hypotonic relative to blood plasma.
⚡ The Role of Flow Rate
Salivary composition depends on how fast saliva is produced.
Low Flow Rate
More time for ductal modification
Greater Na⁺ and Cl⁻ reabsorption
Saliva becomes more hypotonic
High Flow Rate
Less time for modification
Saliva composition is closer to isotonic
This explains why saliva composition changes during eating, stress, or dehydration.
🧠 Functional Importance of Saliva Components
Each component of saliva has a specific role:
Water → Lubrication and swallowing
Bicarbonate (HCO₃⁻) → Buffers acids
Potassium (K⁺) → Electrolyte balance
Reduced Na⁺ and Cl⁻ → Maintains hypotonicity
Saliva supports digestion, protects tooth enamel, and maintains oral pH balance.
🩺 Clinical Relevance
Understanding salivary secretion is important in:
Sjögren syndrome (reduced salivary production)
Cystic fibrosis (chloride transport abnormalities)
Dehydration
Electrolyte imbalances
This concept is frequently tested in:
MCAT
USMLE
Physiology exams
Nursing and allied health exams
📊 Summary Table: Salivary Composition and Secretion
| Feature | Acinar Cells (Initial Secretion) | Ductal Cells (Modification) | Final Saliva |
|---|---|---|---|
| Fluid Type | Isotonic, plasma-like | Modified fluid | Hypotonic |
| Na+ | Secreted (High) | Reabsorbed | Low |
| Cl− | Secreted (High) | Reabsorbed | Low |
| K+ | Low | Secreted | Higher |
| HCO3− | Low | Secreted | Higher |
| Water Movement | Moves freely | Cannot follow solute reabsorption | Remains |
| Osmolarity | Similar to plasma | Decreasing | Lower than plasma |
🎯 Summary
Saliva formation occurs in two stages:
Acinar cells produce isotonic plasma-like fluid
Ductal cells reabsorb Na⁺/Cl⁻ and secrete K⁺/HCO₃⁻
Water does not follow → final saliva becomes hypotonic
In short:
Isotonic at the acinus → Hypotonic at the mouth

Frequently Asked Questions (FAQs)
-
Aim for 4-6 focused hours, ensuring you incorporate breaks to avoid burnout.
-
Practice mindfulness techniques, take practice exams under realistic conditions, and maintain a balanced lifestyle.
-
Set short-term goals, seek support from mentors, and reward yourself for small achievements.
-
Regular exercise improves focus, reduces stress, and enhances overall mental clarity.
-
KOTC offers personalized learning tools, gamification features, and adaptive question banks to help students stay on track without burnout.