
✅ Understanding the Mechanism of SIADH Pathophysiology
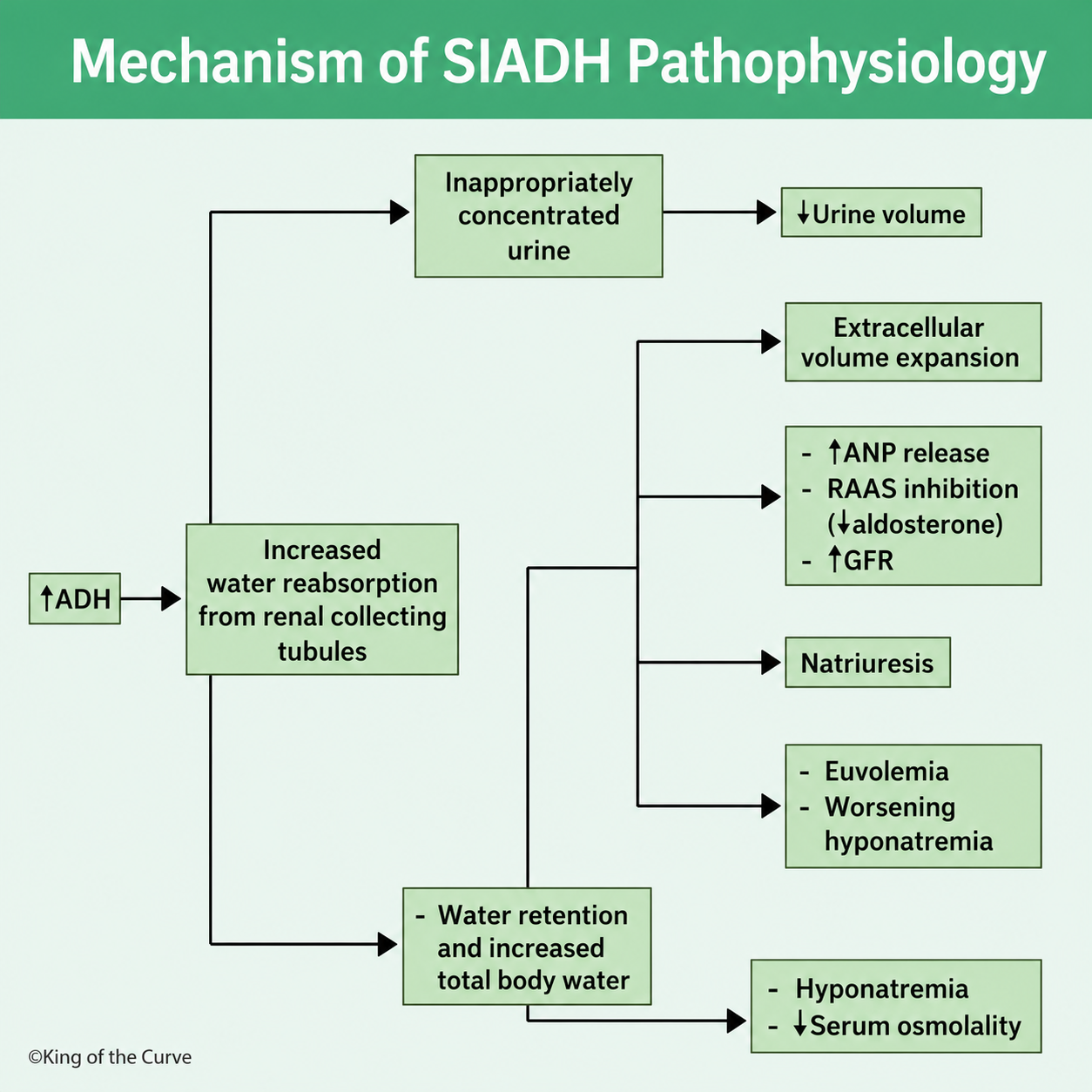
The Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH) is a disorder characterized by the excessive release of antidiuretic hormone (ADH), also known as vasopressin, despite normal or low plasma osmolality. This inappropriate hormone secretion causes the kidneys to retain water, leading to dilutional hyponatremia while maintaining a nearly normal extracellular fluid volume. The infographic above outlines the sequence of events responsible for the development of SIADH.
💧 Excess ADH Increases Water Reabsorption
The hallmark of SIADH is persistent elevation of ADH, which acts on the collecting tubules of the kidneys. ADH increases the insertion of aquaporin-2 water channels into the tubular cells, allowing more water to be reabsorbed back into the bloodstream. Because water is retained without a proportional increase in sodium, total body water rises while serum sodium concentration becomes diluted.
🚰 Concentrated Urine Despite Hyponatremia
Normally, low plasma osmolality suppresses ADH secretion and promotes the excretion of dilute urine. In SIADH, however, ADH remains elevated regardless of plasma osmolality. As a result, the kidneys continue producing inappropriately concentrated urine with reduced urine volume. This inability to excrete free water is one of the defining laboratory findings in SIADH.
📈 Expansion of Extracellular Fluid Volume
Water retention initially produces a mild expansion of the extracellular fluid (ECF) volume. Although this increase is relatively modest, it activates compensatory mechanisms designed to restore fluid balance. These adaptive responses prevent significant edema but contribute to the electrolyte abnormalities characteristic of SIADH.
⚖️ Compensatory Hormonal Responses
The slight increase in extracellular volume stimulates the release of atrial natriuretic peptide (ANP) while suppressing the renin-angiotensin-aldosterone system (RAAS). Aldosterone secretion decreases, reducing sodium reabsorption in the distal nephron. At the same time, the glomerular filtration rate (GFR) may increase slightly, promoting additional sodium excretion.
🧂 Natriuresis Worsens Hyponatremia
The combined effects of elevated ANP, reduced aldosterone, and increased GFR produce natriuresis, meaning excessive urinary sodium loss. Although sodium is lost, water retention continues because ADH remains active. Consequently, the plasma sodium concentration falls further, worsening dilutional hyponatremia.
⚠️ Euvolemic Hyponatremia Develops
Despite retaining water, most patients with SIADH appear euvolemic rather than fluid overloaded. The compensatory loss of sodium and water offsets much of the initial volume expansion, preventing peripheral edema. However, serum sodium continues to decline because the retained water exceeds the amount of sodium remaining in the body.
🧪 Laboratory Findings in SIADH
Typical laboratory features include low serum sodium, decreased serum osmolality, concentrated urine, elevated urine osmolality, and high urine sodium concentration. These findings distinguish SIADH from conditions such as dehydration, heart failure, or cirrhosis, where sodium retention mechanisms are activated instead of suppressed.
📋 Summary of SIADH Pathophysiology
| Step | Physiological Event | Clinical Consequence |
|---|---|---|
| Increased ADH Secretion | Increased water reabsorption in the collecting tubules | Water retention |
| Persistent ADH Activity | Concentrated urine with reduced urine volume | Inability to excrete free water |
| Water Retention | Mild extracellular fluid volume expansion | Activation of compensatory mechanisms |
| Increased ANP and Decreased RAAS | Increased sodium excretion, also called natriuresis | Further sodium loss |
| Continued Water Retention | Dilution of plasma sodium | Hyponatremia and low serum osmolality |
| Compensatory Sodium Loss | Near-normal extracellular fluid volume | Euvolemic hyponatremia |
🩺 Clinical Significance
Recognizing the pathophysiology of SIADH is essential for accurate diagnosis and effective management. Patients typically present with euvolemic hyponatremia, low serum osmolality, concentrated urine, and elevated urine sodium. Treatment focuses on addressing the underlying cause, restricting fluid intake, and using therapies such as hypertonic saline, oral urea, vasopressin receptor antagonists, or loop diuretics in selected patients. Understanding each step of the mechanism helps clinicians interpret laboratory findings and tailor treatment to prevent complications such as cerebral edema and osmotic demyelination syndrome.

Frequently Asked Questions (FAQs)
-
Aim for 4-6 focused hours, ensuring you incorporate breaks to avoid burnout.
-
Practice mindfulness techniques, take practice exams under realistic conditions, and maintain a balanced lifestyle.
-
Set short-term goals, seek support from mentors, and reward yourself for small achievements.
-
Regular exercise improves focus, reduces stress, and enhances overall mental clarity.
-
KOTC offers personalized learning tools, gamification features, and adaptive question banks to help students stay on track without burnout.