
🧠 Dorsal Column–Medial Lemniscus Pathway (DCML): Anatomy & Function
The Dorsal Column–Medial Lemniscus (DCML) pathway is a major sensory pathway responsible for transmitting fine touch, vibration, pressure, and conscious proprioception from the body to the brain. It is essential for precise sensory discrimination, such as identifying textures, detecting vibrations, and maintaining body position awareness.
📍 Pathway Overview
The DCML pathway involves a three-neuron chain:
First-order neuron
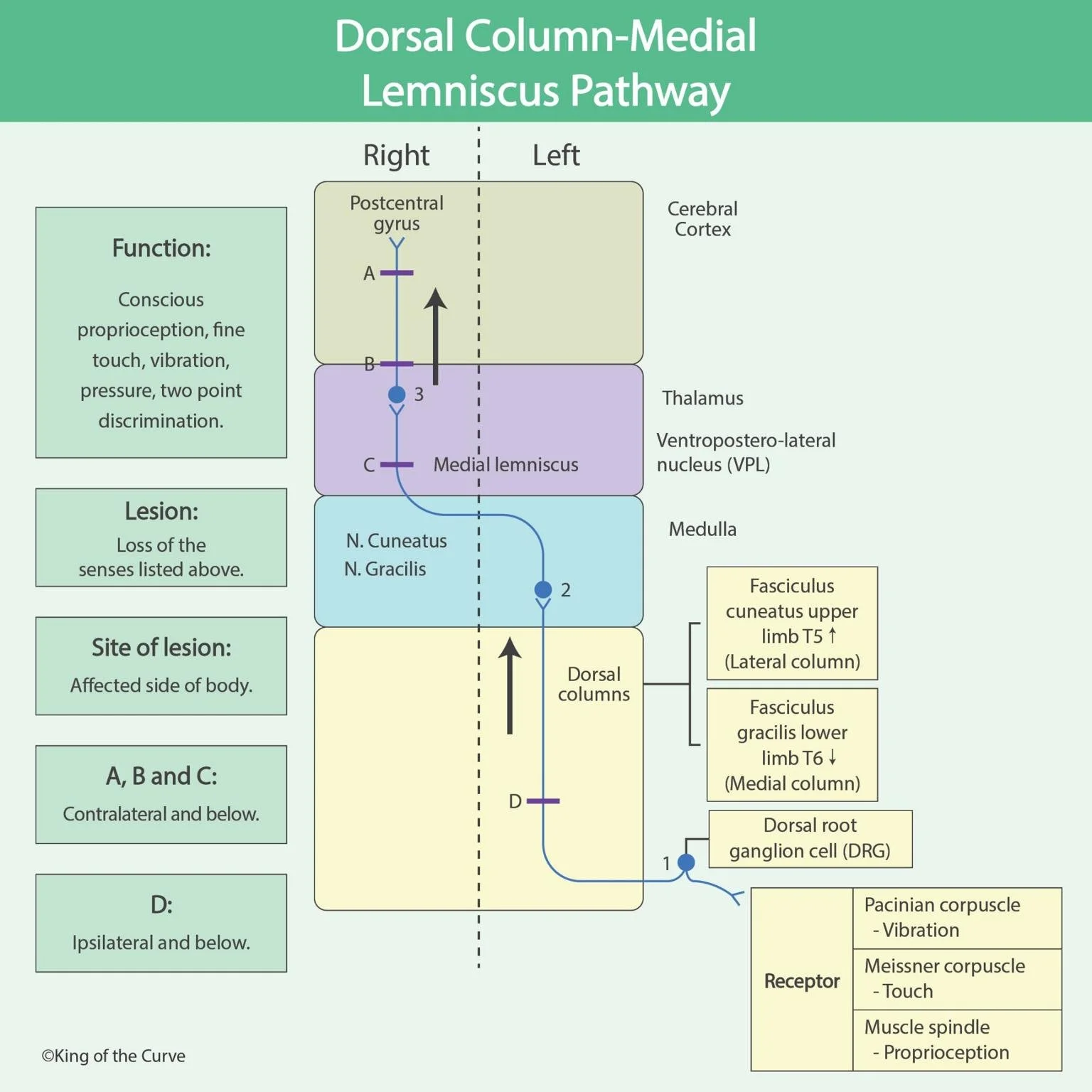
Sensory receptors (e.g., Meissner corpuscles, Pacinian corpuscles, muscle spindles) detect stimuli. Signals travel via peripheral nerves to the dorsal root ganglion (DRG) and then ascend ipsilaterally in the dorsal columns:Fasciculus gracilis → lower body (below T6)
Fasciculus cuneatus → upper body (above T6)
Second-order neuron
These neurons are located in the nucleus gracilis and nucleus cuneatus in the medulla. Here, fibers decussate (cross over) to the opposite side and ascend as the medial lemniscus.Third-order neuron
Signals reach the ventral posterolateral (VPL) nucleus of the thalamus, then project to the postcentral gyrus (primary somatosensory cortex) for conscious perception.
⚙️ Key Functions
The DCML pathway carries:
Fine (discriminative) touch
Vibration sense
Pressure sensation
Conscious proprioception
Two-point discrimination
These modalities allow precise spatial and temporal sensory processing.
🔁 Decussation and Clinical Importance
A key feature of the DCML pathway is that crossing (decussation) occurs in the medulla, not the spinal cord. This has important clinical implications:
Lesions above the medulla → contralateral sensory loss
Lesions below the medulla (spinal cord) → ipsilateral sensory loss
This distinction helps localize neurological lesions.
⚠️ Lesion Patterns
The diagram highlights lesion levels (A, B, C, D) and their effects:
A, B, C (above decussation) → contralateral loss of fine touch, vibration, and proprioception
D (below decussation) → ipsilateral loss of these sensations
Damage to this pathway results in loss of precise sensory input, affecting coordination and balance.
🧪 Clinical Correlations
Common conditions affecting the DCML pathway include:
Vitamin B12 deficiency (Subacute combined degeneration)
Tabes dorsalis (neurosyphilis)
Spinal cord compression or trauma
Patients may present with:
Loss of vibration and position sense
Positive Romberg sign
Sensory ataxia
📊 Summary Table
| Level of Lesion | Location | Sensory Loss |
|---|---|---|
| Above medulla (A, B, C) | Brainstem / Cortex | Contralateral |
| Below medulla (D) | Spinal cord | Ipsilateral |
| Peripheral receptors | Skin / muscles | Localized sensory loss |
🧩 Key Takeaway
The DCML pathway is crucial for high-precision sensory processing and differs from other pathways (like spinothalamic) in both function and site of decussation. Understanding its anatomy is essential for accurately diagnosing neurological lesions.

Frequently Asked Questions (FAQs)
-
Aim for 4-6 focused hours, ensuring you incorporate breaks to avoid burnout.
-
Practice mindfulness techniques, take practice exams under realistic conditions, and maintain a balanced lifestyle.
-
Set short-term goals, seek support from mentors, and reward yourself for small achievements.
-
Regular exercise improves focus, reduces stress, and enhances overall mental clarity.
-
KOTC offers personalized learning tools, gamification features, and adaptive question banks to help students stay on track without burnout.