
🧠 Understanding Pyloric Stenosis for the MCAT
Pyloric stenosis is a high yield gastrointestinal condition that appears frequently in MCAT passages because it integrates anatomy, physiology, clinical presentation, and fluid electrolyte balance. This disorder occurs when the pyloric sphincter muscle becomes hypertrophied, narrowing the gastric outlet and preventing stomach contents from passing into the duodenum. King of the Curve’s visual helps break down both the anatomy and the clinical implications in a clear, digestible way.
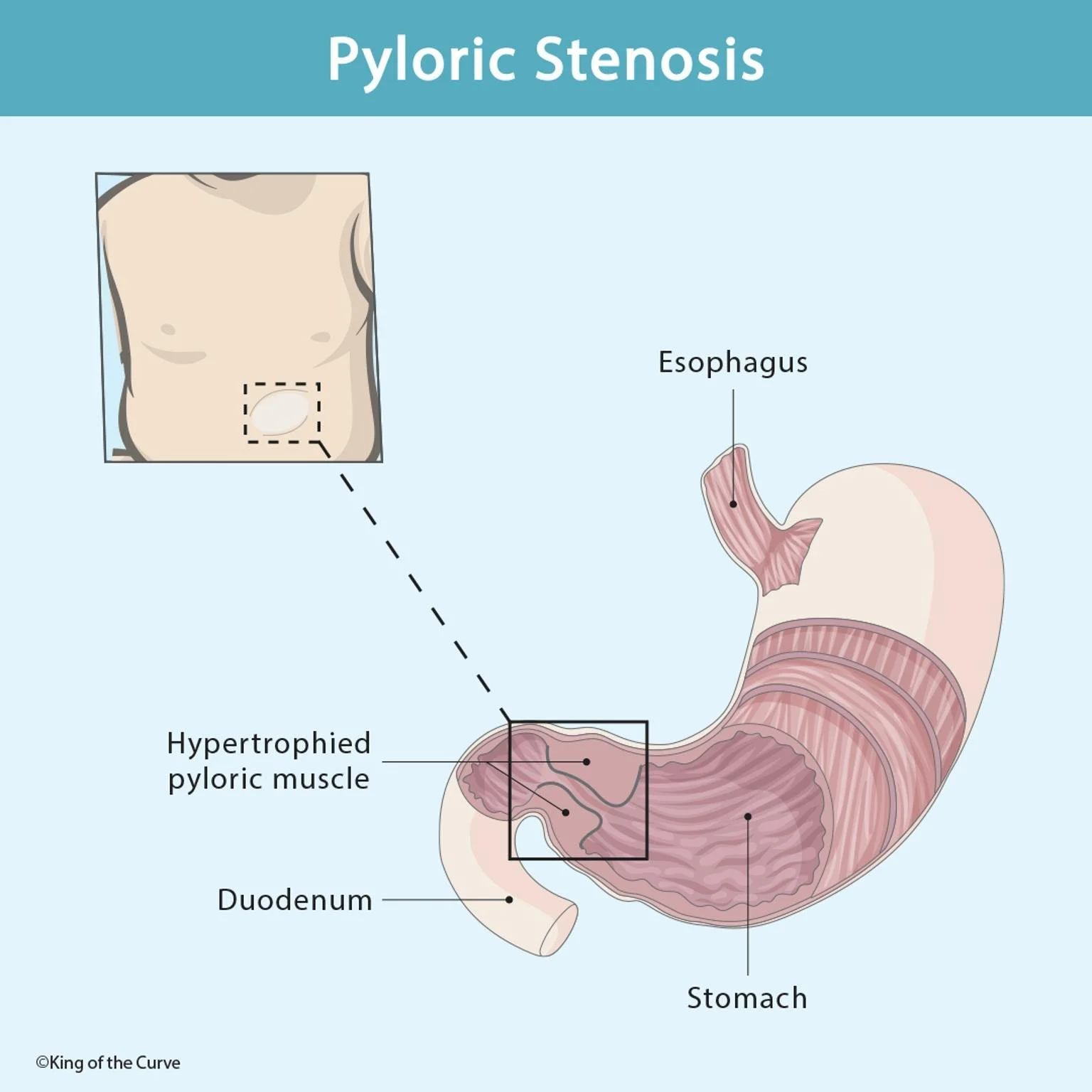
🔍 What Pyloric Stenosis Looks Like Anatomically
The pylorus is the muscular valve that regulates the flow of food from the stomach into the small intestine. In pyloric stenosis, this muscle thickens significantly, as highlighted in the KOTC diagram. The resulting obstruction means that ingested food cannot move forward and begins to accumulate in the stomach, increasing pressure and triggering one of the hallmark symptoms: projectile, non-bilious vomiting.
👶 Why It Commonly Affects Infants
Pyloric stenosis is most often seen in infants around 2–8 weeks of age. While its exact cause is unknown, factors like family history, male sex, and first-born status increase risk. Because infants rely solely on liquid nutrition and feed frequently, gastric obstruction becomes evident quickly. Parents often report persistent vomiting after feeds and visible peristaltic waves moving across the abdomen as the stomach contracts against the obstruction.
⚡ Clinical Presentation and MCAT-Relevant Physiology
The MCAT frequently tests the physiologic consequences of repeated vomiting. Because infants lose large amounts of gastric acid (rich in hydrogen and chloride ions), pyloric stenosis is classically associated with hypochloremic, hypokalemic metabolic alkalosis. The kidneys attempt to compensate by conserving hydrogen ions, which further alters electrolyte balance. Understanding this pattern helps students answer questions about lab findings, respiratory compensation, or renal mechanisms.
📊 High-Yield Table: Key Features of Pyloric Stenosis
| Feature | Description | MCAT Relevance |
|---|---|---|
| Cause | Hypertrophy of pyloric muscle | Involves GI anatomy and motility |
| Symptoms | Projectile non-bilious vomiting, hunger after vomiting | Differentiates from obstruction distal to bile duct |
| Physical Exam | “Olive-shaped” mass in RUQ, visible peristalsis | High-yield diagnosis clue |
| Electrolyte Changes | Hypochloremic, hypokalemic metabolic alkalosis | Acid–base physiology integration |
| Treatment | Pyloromyotomy | Restores gastric emptying |
🧪 Differentiating From Other Causes of Vomiting
A key MCAT skill is distinguishing pyloric stenosis from conditions with similar symptoms. Vomiting that contains bile suggests an obstruction after the duodenum, which rules out pyloric stenosis immediately. Likewise, infections typically include fever or systemic symptoms. The presence of the unique RUQ “olive” on palpation is one of the strongest clues for pyloric stenosis in a clinical vignette.
📚 Mastering GI Disorders With KOTC Tools
KOTC’s anatomy-rich visuals help lock in concepts like pyloric stenosis by linking the structural change (muscle hypertrophy) with the functional consequences (vomiting and electrolyte imbalance). Pairing this image with the Adaptive Q-Bank, daily questions, and guided science resources at kingofthecurve.org/studyscience can significantly strengthen your physiology recall on test day.

Frequently Asked Questions (FAQs)
-
Aim for 4-6 focused hours, ensuring you incorporate breaks to avoid burnout.
-
Practice mindfulness techniques, take practice exams under realistic conditions, and maintain a balanced lifestyle.
-
Set short-term goals, seek support from mentors, and reward yourself for small achievements.
-
Regular exercise improves focus, reduces stress, and enhances overall mental clarity.
-
KOTC offers personalized learning tools, gamification features, and adaptive question banks to help students stay on track without burnout.