
🩺 Mechanism of Bicarbonate Reabsorption in the Proximal Tubule
The proximal convoluted tubule (PCT) reabsorbs approximately 80–90% of the filtered bicarbonate (HCO₃⁻), making it the primary site for maintaining the body's acid-base balance. Although bicarbonate itself cannot readily cross the apical membrane of tubular epithelial cells, the kidneys use a series of transporters and enzymatic reactions to reclaim it efficiently. This process is essential for preventing excessive bicarbonate loss in urine and maintaining normal blood pH.
🧪 Why Bicarbonate Reabsorption Is Important
Bicarbonate is the body's most important extracellular buffer, helping neutralize excess hydrogen ions (H⁺). Every day, the kidneys filter a large amount of bicarbonate through the glomeruli. If this bicarbonate were not reabsorbed, metabolic acidosis would rapidly develop. The proximal tubule conserves bicarbonate while simultaneously secreting hydrogen ions into the tubular lumen.
🔄 Step 1: Hydrogen Ion Secretion
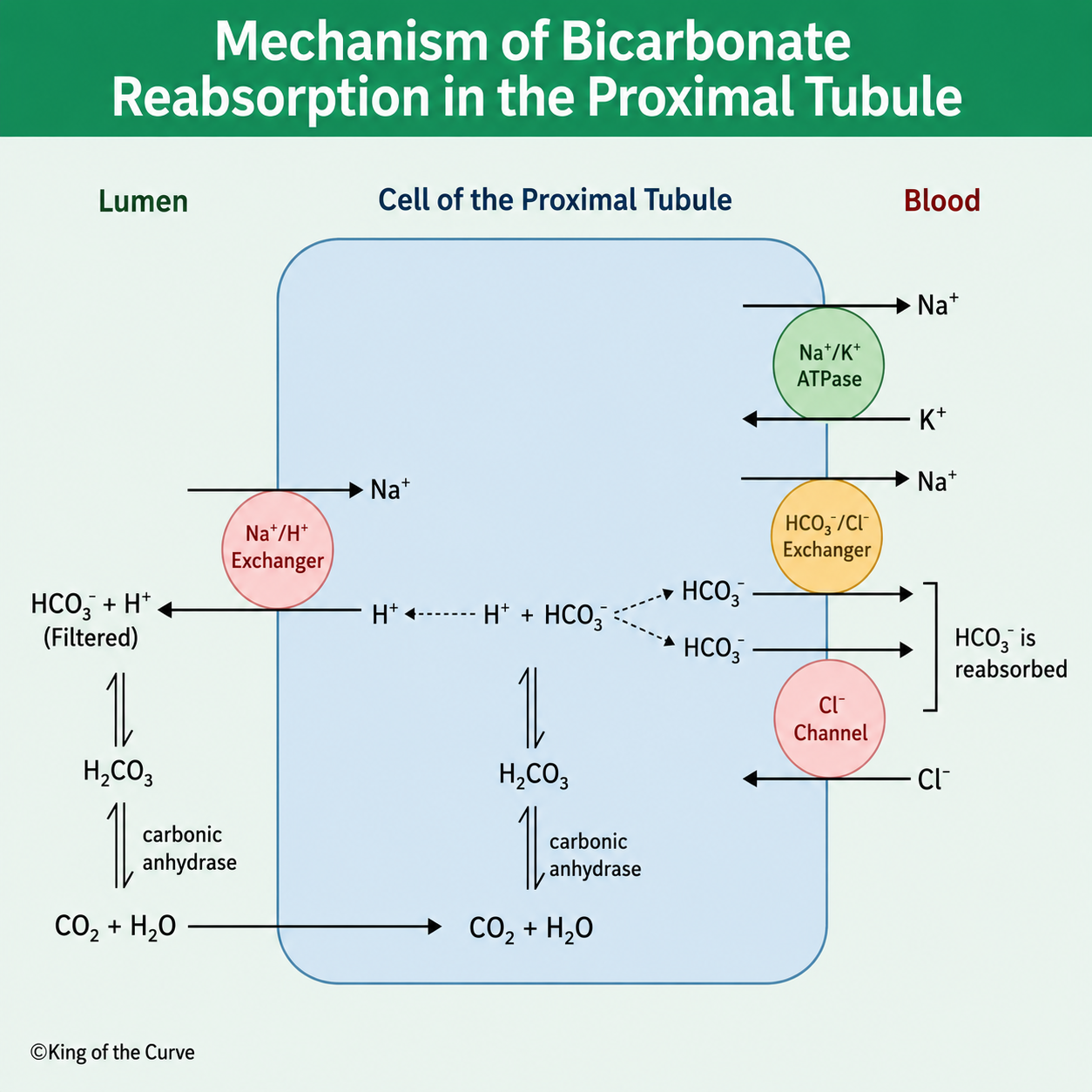
The process begins when the Na⁺/H⁺ exchanger (NHE3) located on the apical membrane transports sodium into the tubular cell while secreting hydrogen ions into the tubular lumen. This exchanger is powered indirectly by the sodium gradient maintained by the Na⁺/K⁺-ATPase on the basolateral membrane.
⚗️ Step 2: Carbonic Anhydrase Converts Filtered Bicarbonate
In the tubular lumen, secreted hydrogen ions combine with filtered bicarbonate to form carbonic acid (H₂CO₃). The enzyme carbonic anhydrase, present on the brush border, rapidly converts carbonic acid into carbon dioxide (CO₂) and water (H₂O). Unlike bicarbonate, carbon dioxide easily diffuses across the cell membrane into the proximal tubular epithelial cell.
🧬 Step 3: Intracellular Regeneration of Bicarbonate
Inside the epithelial cell, intracellular carbonic anhydrase catalyzes the reverse reaction. Carbon dioxide combines with water to reform carbonic acid, which quickly dissociates into hydrogen ions (H⁺) and bicarbonate (HCO₃⁻). The newly generated hydrogen ion is recycled back into the tubular lumen through the Na⁺/H⁺ exchanger, allowing the cycle to continue.
🚚 Step 4: Bicarbonate Moves Into the Blood
The regenerated bicarbonate exits the tubular cell across the basolateral membrane into the bloodstream. This occurs primarily through the Na⁺-HCO₃⁻ cotransporter, while chloride-bicarbonate exchange mechanisms may also contribute depending on the nephron segment. As a result, filtered bicarbonate is effectively returned to the circulation without being directly transported across the apical membrane.
⚙️ Role of the Na⁺/K⁺-ATPase
The Na⁺/K⁺-ATPase located on the basolateral membrane continuously pumps sodium out of the cell and potassium into the cell. This creates the sodium concentration gradient that drives sodium entry through the Na⁺/H⁺ exchanger, making bicarbonate reabsorption possible. Without this pump, sodium transport and hydrogen ion secretion would cease.
💊 Clinical Significance
Several medications, including acetazolamide, inhibit carbonic anhydrase and reduce bicarbonate reabsorption. This results in increased urinary bicarbonate loss, alkaline urine, and mild metabolic acidosis. Carbonic anhydrase inhibitors are commonly used to treat glaucoma, altitude sickness, metabolic alkalosis, and certain forms of epilepsy.
📊 Summary of Bicarbonate Reabsorption in the Proximal Tubule
| Step | Process | Key Components |
|---|---|---|
| 1 | Hydrogen ion secretion into the lumen | Na+/H+ exchanger (NHE3) |
| 2 | Formation and breakdown of carbonic acid | Luminal carbonic anhydrase |
| 3 | CO2 diffuses into the tubular cell | Passive diffusion |
| 4 | Regeneration of HCO3− inside the cell | Intracellular carbonic anhydrase |
| 5 | Bicarbonate is transported into the blood | Na+-HCO3− cotransporter and Na+/K+-ATPase |
✅ Key Takeaway
The proximal tubule conserves nearly all filtered bicarbonate through a coordinated mechanism involving hydrogen ion secretion, carbonic anhydrase activity, carbon dioxide diffusion, and sodium-dependent transporters. This process is fundamental for maintaining acid-base homeostasis and is a common target for pharmacological intervention in several clinical conditions.

Frequently Asked Questions (FAQs)
-
Aim for 4-6 focused hours, ensuring you incorporate breaks to avoid burnout.
-
Practice mindfulness techniques, take practice exams under realistic conditions, and maintain a balanced lifestyle.
-
Set short-term goals, seek support from mentors, and reward yourself for small achievements.
-
Regular exercise improves focus, reduces stress, and enhances overall mental clarity.
-
KOTC offers personalized learning tools, gamification features, and adaptive question banks to help students stay on track without burnout.