
🧠 Malignant Hyperthermia: Pathomechanisms & Therapy
Malignant Hyperthermia (MH) is a rare, life-threatening pharmacogenetic reaction to certain anesthetics. A sudden, uncontrolled rise in skeletal-muscle metabolism drives hypercapnia, acidosis, hyperthermia, and rhabdomyolysis. Rapid recognition and treatment are critical.
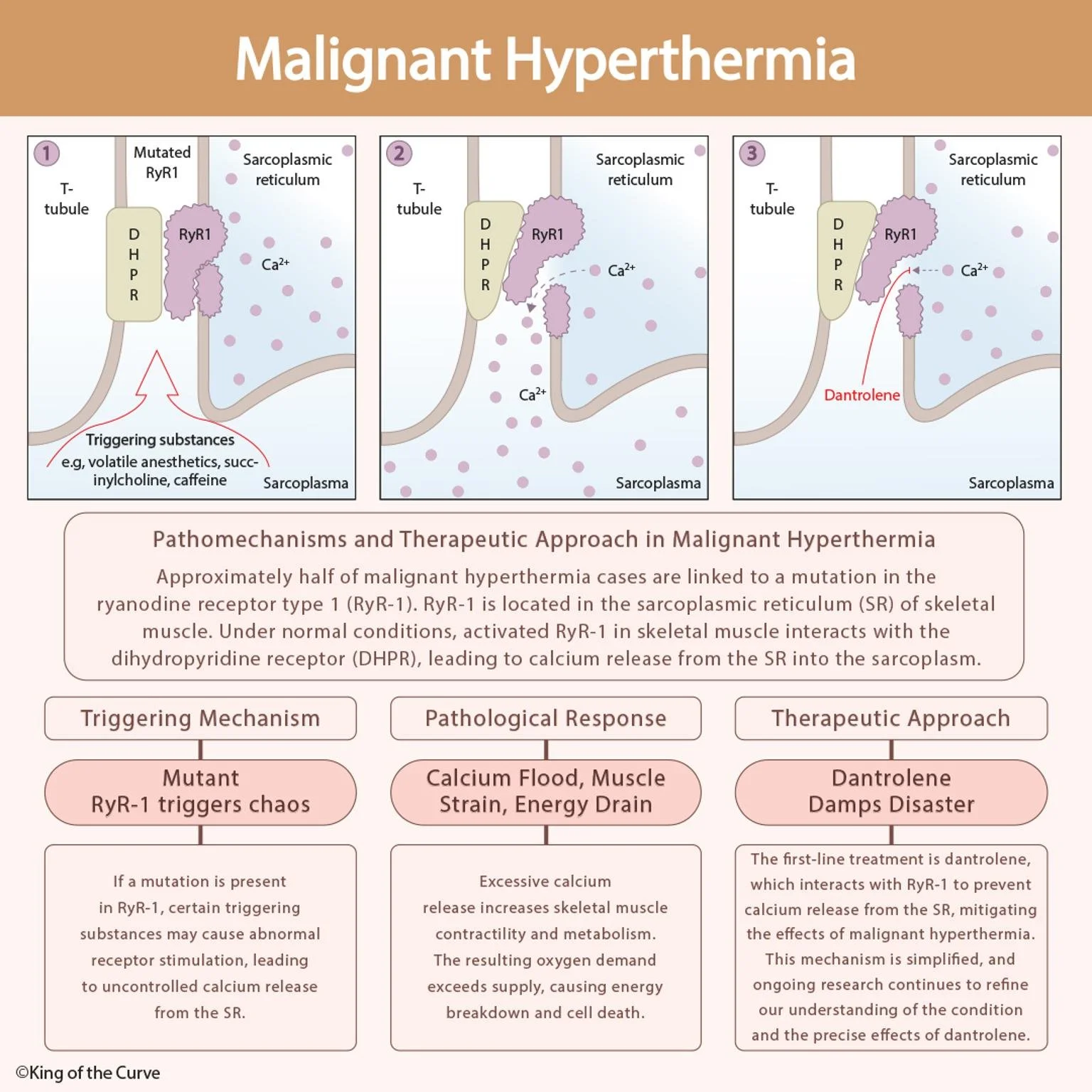
⚙️ The Core Mechanism: RyR1–DHPR Misfire
Under normal physiology, the ryanodine receptor type 1 (RyR1) on the sarcoplasmic reticulum (SR) releases Ca²⁺ when coupled to the dihydropyridine receptor (DHPR) in the T-tubule—initiating contraction.
In MH-susceptible patients, RyR1 mutations make the channel hyperactive. Exposure to triggers (e.g., volatile anesthetics or succinylcholine) causes excessive Ca²⁺ release into the sarcoplasm → relentless contraction → skyrocketing ATP consumption, heat production, and cellular injury.
🩺 What You’ll See Clinically
Early: Unexplained ↑ETCO₂, tachycardia, muscle rigidity (masseter), mixed metabolic/respiratory acidosis
Progression: Rapid hyperthermia, hyperkalemia, myoglobinuria, arrhythmias
Labs: ↑CK, ↑K⁺, dark urine (myoglobin), low bicarbonate/low pH
📊 High-Yield Summary Table
| Aspect | Details |
|---|---|
| Triggering Mechanism | Mutant RyR1 → uncontrolled SR Ca²⁺ release after exposure to volatile agents or succinylcholine |
| Pathological Response | Ca²⁺ flood → sustained contraction, ↑O₂ demand, CO₂ overproduction, heat, rhabdomyolysis |
| Therapeutic Approach | Dantrolene: inhibits SR Ca²⁺ release, halts hypermetabolic crisis |
| Common Triggers | Halothane, isoflurane, sevoflurane; succinylcholine; (lab tests may use caffeine/halothane contracture testing) |
| Key Signs | ↑ETCO₂, rigidity, tachycardia → rising temp, hyperkalemia, myoglobinuria |
| Initial Actions | Stop triggers, call MH protocol, 100% O₂, active cooling, treat acidosis/hyperK⁺, prepare dantrolene |
💊 Dantrolene: The Game-Changer
Dantrolene sodium directly stabilizes RyR1 to reduce SR Ca²⁺ release.
Dose: 2.5 mg/kg IV immediately; repeat to effect (up to ~10 mg/kg)
Support: 100% O₂, cooling (ice packs, chilled IV fluids), treat hyperkalemia (calcium, insulin/glucose), correct acidosis (bicarbonate), monitor for recrudescence (continue dantrolene infusion per protocol)
🧬 Prevention & Screening Pearls
History matters: personal/family MH, adverse anesthetic events, unexplained peri-op hypercapnia/rigidity
Testing: genetic panels (e.g., RYR1, CACNA1S) and/or caffeine–halothane contracture test (CHCT) at specialized centers
Anesthetic planning: use non-triggering regimens (e.g., TIVA with propofol), flush anesthesia machines, remove vaporizers, have dantrolene immediately available
🚀 Call to Action
Master crises before they happen. Explore more concise visuals and high-yield mechanisms with King of the Curve—where complex physiology becomes clear, memorable, and test-ready. Keep building your emergency medicine toolkit with our adaptive Q-bank, daily questions, and visual concept library.

Frequently Asked Questions (FAQs)
-
Aim for 4-6 focused hours, ensuring you incorporate breaks to avoid burnout.
-
Practice mindfulness techniques, take practice exams under realistic conditions, and maintain a balanced lifestyle.
-
Set short-term goals, seek support from mentors, and reward yourself for small achievements.
-
Regular exercise improves focus, reduces stress, and enhances overall mental clarity.
-
KOTC offers personalized learning tools, gamification features, and adaptive question banks to help students stay on track without burnout.