
🧠 Auditory Pathway and Lesion Sites in the Brainstem
The auditory system is a sophisticated neural network that allows us to perceive and interpret sound. This blog post explores the anatomy of the auditory pathway and the impact of lesions at specific sites in the brainstem on hearing.
🎧 Overview of the Auditory Pathway
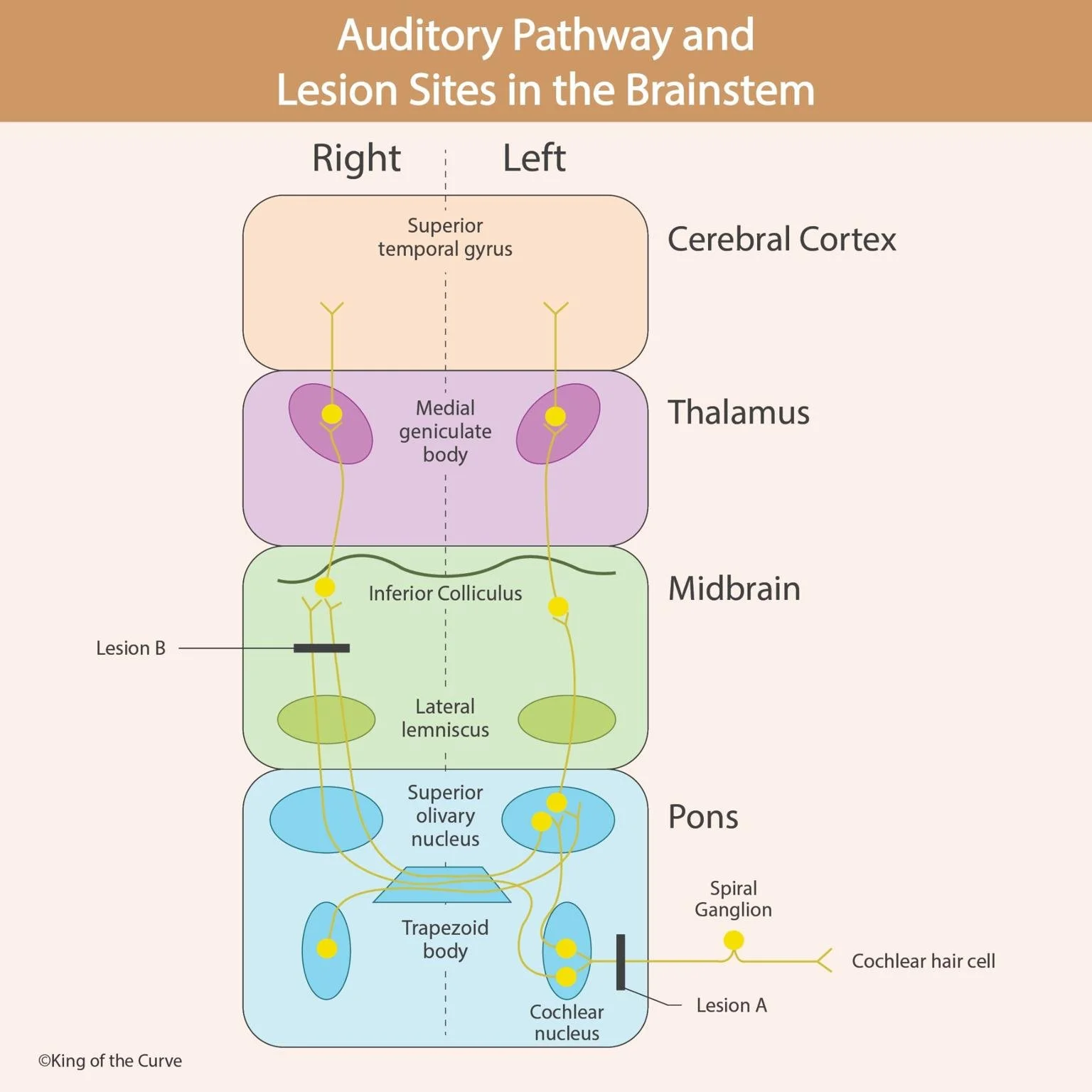
The auditory pathway involves both peripheral and central components. Sound waves are detected by cochlear hair cells in the inner ear and transformed into electrical impulses that travel through a series of relay stations before reaching the auditory cortex for processing.
🔁 Flow of the Auditory Signal
Cochlear Hair Cells: These mechanoreceptors convert sound vibrations into electrical signals.
Spiral Ganglion: Houses the sensory neurons that transmit signals to the brainstem.
Cochlear Nucleus (Pons): First relay station in the brainstem where auditory signals synapse.
Trapezoid Body and Superior Olivary Nucleus: Involved in sound localization and bilateral auditory processing.
Lateral Lemniscus (Midbrain): Carries impulses up to the midbrain.
Inferior Colliculus (Midbrain): Major integrative center for auditory signals.
Medial Geniculate Body (Thalamus): Final relay before auditory information reaches the cerebral cortex.
Superior Temporal Gyrus (Cortex): Location of the primary auditory cortex, where sound perception occurs.
⚠️ Lesion Sites and Their Effects
This diagram highlights two critical lesion sites in the brainstem and their potential clinical outcomes:
❌ Lesion A (at the level of the Cochlear Nucleus)
Effect: Causes ipsilateral sensorineural hearing loss.
Explanation: Since this is early in the auditory pathway (before decussation), damage here affects the same side as the lesion.
Clinical Insight: This type of lesion is rare but often associated with tumors such as acoustic neuromas.
❌ Lesion B (at the level of the Lateral Lemniscus)
Effect: Causes minimal or subtle hearing loss due to bilateral innervation.
Explanation: Because auditory signals cross over early and ascend bilaterally, a lesion at this level is less likely to produce profound hearing deficits.
Clinical Insight: May affect sound localization and auditory reflexes, rather than complete hearing loss.
🏥 Clinical Relevance
Understanding the auditory pathway is critical for diagnosing and managing:
Sensorineural hearing loss
Acoustic neuromas
Brainstem strokes
Auditory processing disorders
Additionally, precise localization of lesions can guide neuroimaging and surgical interventions.
📌 Key Takeaways
The auditory pathway is bilateral, providing redundancy and preserving hearing even when parts of the brainstem are affected.
Lesions in early components (e.g., cochlear nucleus) result in ipsilateral deficits.
Lesions in higher components (e.g., midbrain or thalamus) often result in subtle or no hearing loss, thanks to crossover pathways.

Frequently Asked Questions (FAQs)
-
Aim for 4-6 focused hours, ensuring you incorporate breaks to avoid burnout.
-
Practice mindfulness techniques, take practice exams under realistic conditions, and maintain a balanced lifestyle.
-
Set short-term goals, seek support from mentors, and reward yourself for small achievements.
-
Regular exercise improves focus, reduces stress, and enhances overall mental clarity.
-
KOTC offers personalized learning tools, gamification features, and adaptive question banks to help students stay on track without burnout.