
🩺 HMWH vs LMWH: The Cleanest Way to Remember Heparins
Heparins show up in MCAT biochem/physiology passages and NCLEX pharmacology questions. If you can picture how each type interacts with antithrombin and which labs/reversal to use, you’ll bank fast points and make safer choices at the bedside.
🧬 Mechanism in one line
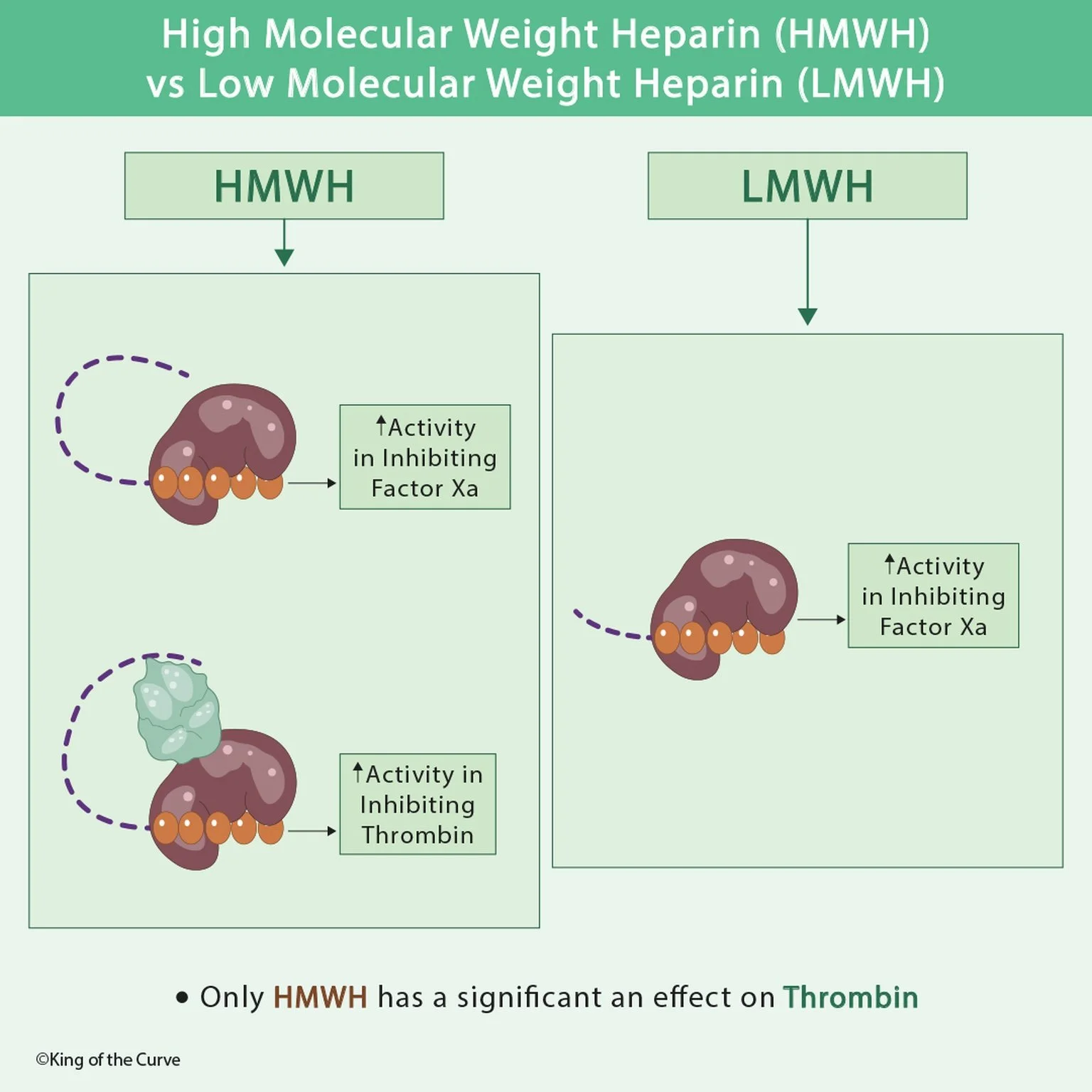
Both HMWH and LMWH potentiate antithrombin.
HMWH (unfractionated heparin) is long enough to bridge antithrombin to thrombin → inhibits IIa + Xa.
LMWH is shorter and can’t bridge to thrombin → primarily inhibits Xa (little IIa activity).
📊 High-Yield Comparison Table
| Feature | HMWH (Unfractionated Heparin) | LMWH (Enoxaparin, Dalteparin) |
|---|---|---|
| Primary targets | Factor Xa + Thrombin (IIa) | Factor Xa (≪ effect on IIa) |
| Mechanistic note | Long chain can bridge antithrombin to thrombin → blocks IIa + Xa | Short chain cannot bridge to thrombin → mainly anti-Xa |
| Monitoring | aPTT for infusions/titration | No routine labs; use anti-Xa in pregnancy, obesity, renal impairment |
| Reversal | Protamine — complete | Protamine — partial |
| Clearance | Hepatic/reticuloendothelial | Renal — dose adjust in CKD |
| Onset/offset | Rapid on/off; short half-life | Longer half-life; predictable levels |
| HIT risk | Present | Lower (not zero) |
| Typical use | ICU/procedures, need tight titration or rapid reversal; severe renal impairment | Outpatient DVT/PE treatment & prophylaxis; pregnancy; cancer-associated thrombosis |
| Route | IV or SQ (often IV infusion inpatient) | SQ; fixed or weight-based dosing |
| Board hook | Meaningful thrombin (IIa) inhibition | Primarily anti-Xa; minimal IIa effect |
Board hook: Only HMWH has a meaningful anti-thrombin (IIa) effect.
🧪 Monitoring & Reversal
HMWH: follow aPTT; reverse with protamine sulfate (complete).
LMWH: typically no monitoring; check anti-Xa when needed; protamine gives partial reversal only.
⚠️ Adverse effects you must connect
Bleeding (both).
HIT (heparin-induced thrombocytopenia): immune thrombosis 5–10 days after heparin exposure → stop all heparins, start non-heparin anticoagulant (e.g., argatroban, bivalirudin; fondaparinux option).
Osteoporosis with long-term HMWH.
Renal accumulation with LMWH → bleeding if not dose-adjusted.
🧠 MCAT & NCLEX Quick Hits
Mechanism check: Heparins ↑ antithrombin (don’t confuse with warfarin → vitamin K epoxide reductase inhibition).
Lab pairing: HMWH ↔ aPTT; warfarin ↔ PT/INR; LMWH ↔ anti-Xa (selected cases).
Renal function steers you toward HMWH when eGFR is very low.
🧩 Mini Practice (fast answers below)
Best outpatient DVT treatment during pregnancy?
Massive bleed on UFH—reversal?
eGFR 20 mL/min on LMWH—what change?
Which agent does not significantly inhibit thrombin?
Keys: 1) LMWH (enoxaparin); 2) Protamine sulfate (complete); 3) Switch to HMWH or dose-reduce with monitoring; 4) LMWH.
🚀 Keep climbing the curve
(Place the KOTC logo here before your CTA.)
Daily warm-ups: kingofthecurve.org/qotd
Visual library: kingofthecurve.org/studyscience
Start free: kingofthecurve.org/free-lifetime | Book trial sessions
Premed hub: kingofthecurve.org/pre-med-essentials

Frequently Asked Questions (FAQs)
-
Aim for 4-6 focused hours, ensuring you incorporate breaks to avoid burnout.
-
Practice mindfulness techniques, take practice exams under realistic conditions, and maintain a balanced lifestyle.
-
Set short-term goals, seek support from mentors, and reward yourself for small achievements.
-
Regular exercise improves focus, reduces stress, and enhances overall mental clarity.
-
KOTC offers personalized learning tools, gamification features, and adaptive question banks to help students stay on track without burnout.