
👀 Frontal Eye Fields & Horizontal Gaze — A High-Yield Guide (MCAT/NCLEX)
Neuro eye-movement questions show up every MCAT cycle and in NCLEX neuro checks. If you can picture how the frontal eye fields (FEF) drive the brainstem gaze centers to move both eyes together, you’ll localize lesions in seconds and avoid classic traps (INO, PPRF vs VI nucleus, “one-and-a-half” syndrome).
🧠 What the Frontal Eye Fields Do
Location: Premotor cortex, Area 8.
Job: Initiate saccades toward the contralateral side by activating the contralateral PPRF (horizontal gaze center).
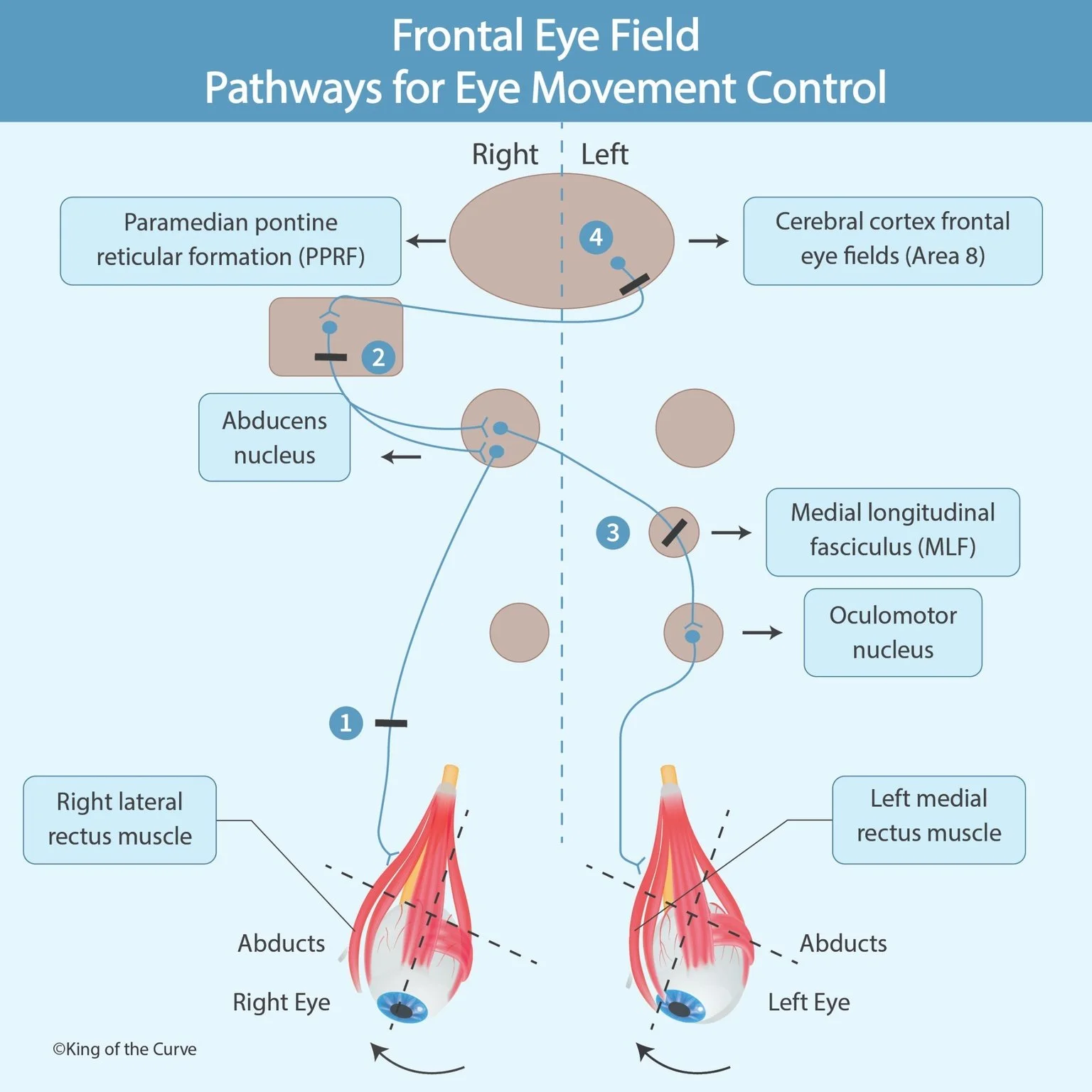
🧭 The 4-Step Pathway (left gaze example)
Right FEF → Left PPRF (contralateral drive).
Left PPRF → Left abducens nucleus (VI) to abduct left eye (left lateral rectus).
Abducens internuclear neurons → MLF to right oculomotor nucleus (III) → adduct right eye (right medial rectus).
Result: Conjugate leftward gaze (both eyes look left).
📊 Lesions & Findings (print-friendly table)
| Lesion | Primary Deficit | Signature Finding | Exam Angle |
|---|---|---|---|
| Frontal Eye Field (cortical) | Poor contralateral saccades | Eyes deviate toward the lesion acutely | Stroke localizer; cortical control |
| PPRF (horizontal gaze center) | Ipsilateral gaze palsy of both eyes | Can’t look toward the lesion | Brainstem lesion vs nerve palsy |
| Abducens nucleus (VI nucleus) | Ipsilateral gaze palsy (same as PPRF) | Often + facial nerve signs (nearby) | Pontine lesion nuance |
| MLF (internuclear) | Internuclear ophthalmoplegia (INO) | Ipsilateral eye can’t adduct; other eye has abducting nystagmus; convergence spared | MS vignette; “internuclear” keyword |
| PPRF/VI + MLF (same side) | One-and-a-half syndrome | Only the contralateral eye abducts | Classic boards favorite |
Need a styled Squarespace table? Say the word and I’ll drop in the combined HTML/CSS block.
🧪 Mini Practice (MCAT-style)
Eyes deviate right after a stroke; patient struggles to look left. Lesion?
On left gaze, the right eye won’t adduct; left eye shows abducting nystagmus; convergence intact. Diagnosis?
Patient can’t look right with either eye; vertical movements intact. Where’s the lesion?
Keys: (1) Right FEF. (2) Right INO from right MLF lesion. (3) Right PPRF or right abducens nucleus.
🧩 Pattern Recognition Tips
“Convergence spared” → think INO/MLF (medial rectus works via a different pathway).
Gaze palsy of both eyes toward one side → PPRF or VI nucleus on that side.
Initial gaze deviation toward the lesion in acute cortical strokes → FEF.
🚀 Keep climbing the curve with KOTC
Daily warm-up: kingofthecurve.org/qotd
Visual library: kingofthecurve.org/studyscience
Try Free Lifetime or book trial sessions
Premed hub: kingofthecurve.org/pre-med-essentials

Frequently Asked Questions (FAQs)
-
Aim for 4-6 focused hours, ensuring you incorporate breaks to avoid burnout.
-
Practice mindfulness techniques, take practice exams under realistic conditions, and maintain a balanced lifestyle.
-
Set short-term goals, seek support from mentors, and reward yourself for small achievements.
-
Regular exercise improves focus, reduces stress, and enhances overall mental clarity.
-
KOTC offers personalized learning tools, gamification features, and adaptive question banks to help students stay on track without burnout.